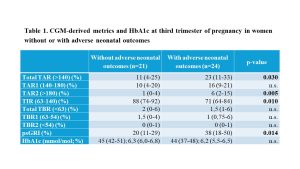
Background and aims: The Glycemia Risk Index (GRI) describes the quality of glycemic control, emphasizing extreme hypo- and hyperglycemia more than less extreme values. However, a pregnancy-specific GRI (psGRI), tailored to the tighter glucose target range required during pregnancy, has not been established. Materials and methods: We prospectively evaluated clinical, metabolic, and CGM data across pregnancy, in pregnant women with insulin-treated diabetes, managed between September 2021 and March 2024 in our Diabetes Unit. We defined first and second levels of hyperglycemia (TAR1: 140-180 mg/dL, TAR2: >180 mg/dL) and hypoglycemia (TBR1: 63-54 mg/dL, TBR2: <54 mg/dL), to calculate the psGRI at each trimester (using the GRI calculator available online). Logistic regression analysis was performed to examine the association between psGRI and the risk of adverse neonatal outcomes (including neonatal hypoglycemia, jaundice, LGA, SGA, preterm delivery, NICU admission). Results: Overall, 45 pregnant women with diabetes treated with multiple daily insulin injection were evaluated (20 T1D, 17 T2D, and 8 GDM; age: 34±4 years, pre-pregnancy BMI: 26±5 kg/m2, gestational weight gain: 11±5 kg). Of these, 24 (53%) experienced at least one adverse outcome (75% in women with T1D vs 36% in T2D and GDM women, p=0.020). In the third trimester of pregnancy (Tab. 1), despite similar HbA1c levels, women with adverse outcomes had significantly higher total TAR (>140 mg/dL) and lower TIR (63-140 mg/dL). Specifically, within the hyperglycemic range, the difference was seen in TAR2, whereas TAR1 was comparable between the two groups. This difference was reflected in the higher psGRI observed in women with adverse neonatal outcomes. Logistic regression analysis showed that third trimester psGRI slightly but significantly increased the risk of adverse neonatal outcomes (OR: 1.046 [1.006-1.087], p=0.025). Conclusions: Pregnant women with insulin-treated diabetes reporting adverse neonatal outcomes spent more time in hyperglycemia, particularly in extreme hyperglycemia (>180 mg/dL), compared to those without adverse outcomes. Therefore, the level of hyperglycemia should always be assessed during pregnancy. The psGRI, placing greater emphasis on extreme hyperglycemia, may be a novel comprehensive tool for assessing the risk of adverse neonatal outcomes in these women. Supported by PNRR-M4C2-1.3, Project PE_00000019 HEAL ITALIA.