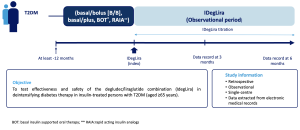
Background and aims: This is an interim evaluation of the STOP study (Simplifying Treatment in Older People), a proof-of-concept observation, whose aim is to test effectiveness and safety of IDegLira in deintensifying diabetes therapy in insulin-treated persons with T2DM aged >65 years. Materials and methods: The study, retrospective observational, gathered so far data related to 93 consecutive persons with T2DM, in whom IDegLira was introduced in therapy, and for whom clinical data were available for at least 6 months after the switch. Results: The 93 persons (42 F, age 76±8 yrs, diabetes duration 20±10 yrs, duration of insulin treatment 13±12 yrs, BMI 28.6±4.9 kg/m2, A1C 7.4±0.9), were for the 75% in basal/bolus insulin therapy. Sixteen % of them, needed caregiver, whereas 53% were in follow-up at the Geriatric Clinic for mild/severe cognitive impairment. After 3 months, fasting plasma glucose (PG) decreased (from 138±38 to 117±24 mg/dl, p=0.000036 vs baseline), similarly A1C (from 7.4±0.9 to 7.0±0.6%, p=0.000126). All results showed additional improvement at 6 month (p<0.005 vs baseline). Rates of hypoglycemia at any time of day (PG<70 mg/dl) were lower after 3 months (0.35±0.94 vs 1.15±2.61, episodes/pt/month, p=0.0057). Episodes with PG<54 mg/dl decreased (from 0.56±1.71 to 0.03±0.25, p=0.0093). Accordingly, the proportion of patients with at least one episode of PG<70 mg and 54 mg/dl, felt down from baseline to 3 month (23.7 to 14%;16.1 to 11%, respectively), being zero at 6 months. Rapid acting insulin dose decreased by 80% at 3, up to 95% at 6 months (from 0.18±0.13 to 0.04±0.06 at 3, and 0.01±0.04 U/kg at 6 months, p<0.0001). Nearly all patients interrupted it. IDegLira was initiated at a mean dose of 17±5.4 U/die to further increase to 23±9.6 after 6 months. BMI did not change significantly (p=ns). Conclusion: According to our preliminary results, IDegLira seems to offer a relevant option, to more complex insulin regimens, in terms of effectiveness and safety, in a population in whom preventing hypoglycemia and improving quality of life are mandatory and clinical inertia is often present.